Disclaimer
The information provided pertains to specimen collection and laboratory testing requests and is intended solely as a general example for procedural documentation purposes. It does not constitute medical or legal advice and should not replace consultation with qualified healthcare or legal professionals. Variations in regulations and requirements may exist across different jurisdictions, and modifications might be necessary to ensure proper compliance. The use of this example is at the user’s own risk, and no liability is assumed for any errors, omissions, or adverse outcomes resulting from its application without appropriate professional review.
Please note: This is a sample template of a Lab Requisition Form US, intended for reference purposes only. Actual forms may vary depending on institutional requirements and regulations.
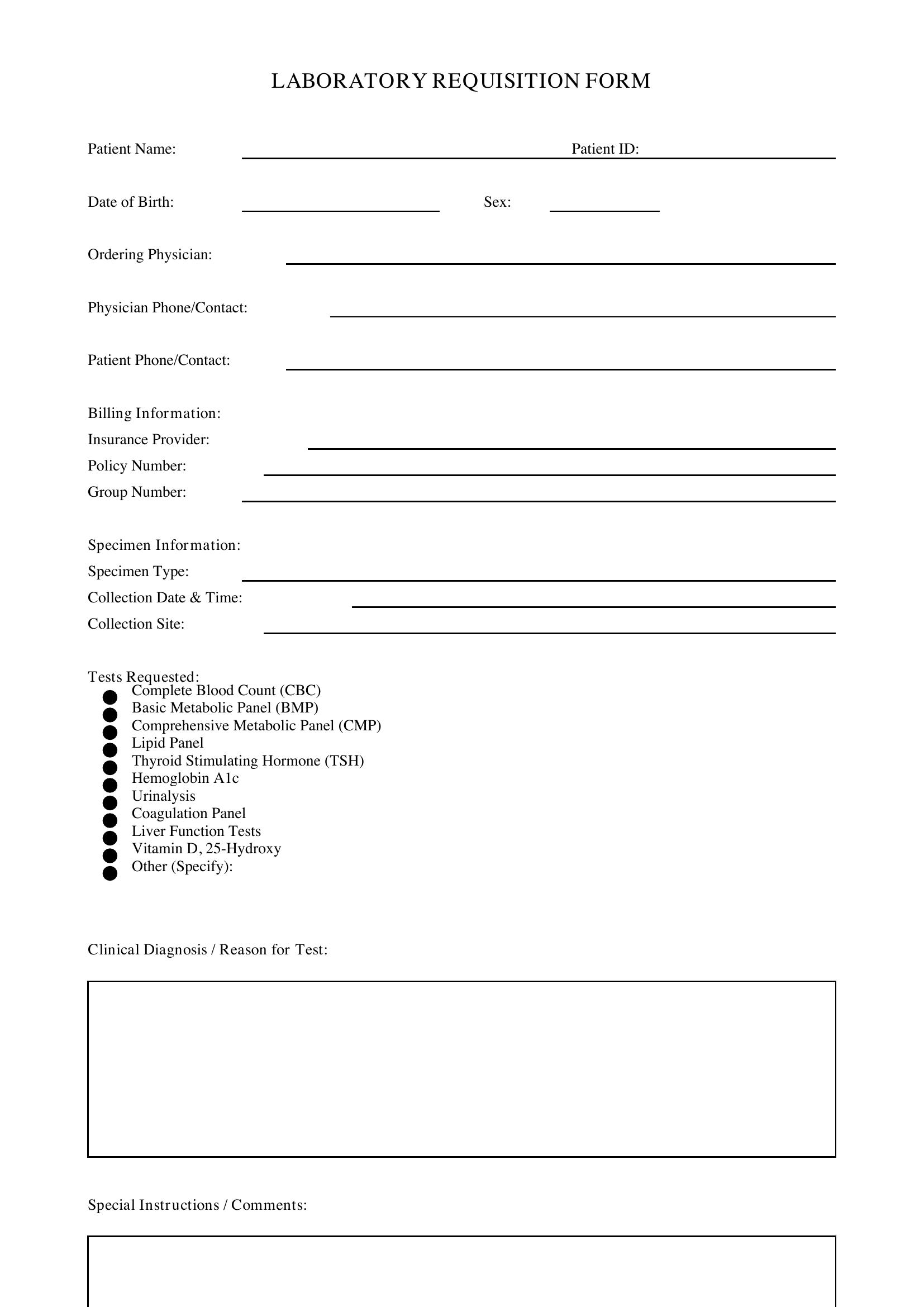
Lab Requisition Form US Sample
Requisition Details:
Requisition Number: ______________________
Date of Request: ______________________
Patient Information:
Name: ______________________
Date of Birth: ______________________
Gender: ______________________
Address: ______________________
Referring Provider:
Name: ______________________
Department/Title: ______________________
Contact Information: ______________________
Tests Requested:
- Test 1: ______________________
- Test 2: ______________________
- Additional Tests: ______________________
Sample Collection:
Sample Type: ______________________
Collection Date & Time: ______________________
Collection Location: ______________________
Special Instructions:
Please specify any special handling or instructions here.
Authorized Signature: ______________________
Date: ______________________
Location: ______________________
Date: ______________________
Provider Signature
Lab Technician